How Do Dentists Fix a Broken Tooth? A Steady, Straightforward Guide You Can Rely On
Cracking a tooth can make your stomach drop. The upside: today’s dentistry can handle almost every type of break. Most fixes are gentler, quicker, and more lifelike than you might expect.
- Get same‑day care if you have intense pain, swelling, fever, heavy bleeding, a tooth that’s been knocked out, or a deep post‑injury crack. Time matters.
Table of Contents
What “broken tooth” really means
Some breaks dive all the way to the nerve. The ideal solution depends on the depth of damage, whether the pulp is involved, and if the fracture extends beneath the gumline. Your dentist will tailor the plan to those details.
- Typical fracture types include:
- Small chip or corner fracture.
- Craze lines (superficial enamel cracks).
- Cusp fracture (one of the tooth’s peaks snaps off).
- Cracked tooth (a line that travels toward or into the nerve chamber).
- Split tooth (the tooth divides into separate pieces).
- Root fracture (below the gumline).
First aid before you see the dentist
Rinse with warm water, gently. If you’re bleeding, hold clean gauze with firm pressure. Over‑the‑counter pain medicine can help. If a sharp edge irritates your cheek or tongue, cover it with dental wax or sugar‑free gum. Breathe. Most cases are fixable.
- Do and don’t:
- Do save any broken piece in milk or saline.
- Do avoid very hot, cold, or sweet foods.
- Don’t chew on the broken side.
- Don’t use glue or aspirin on the tooth or gums.
How dentists figure out the right fix
Your dentist will listen first. Then they’ll examine, test the bite, shine light through the tooth, and take X‑rays. Sometimes 3D imaging or a fiber‑optic transillumination is used to trace a crack.
- Diagnostic tools your dentist may use:
- Bite stick tests to locate pain.
- Cold or air tests to check the nerve.
- Periapical or bitewing X‑rays to see bone and decay.
- Cone beam CT for complex or root fractures.
- Intraoral photos to monitor and explain.

Your options at a glance
Here’s a down‑to‑earth snapshot. Prices and timelines differ by location and insurance, but these ranges mirror typical U.S. estimates.
| Situation | Best-fit treatment | What it does | Visits | Comfort | Typical lifespan | US ballpark cost |
|---|---|---|---|---|---|---|
| Tiny chip, smooth edges | Recontouring + polish | Shapes enamel only | 1 | Very easy | Permanent | $0–$150 |
| Small chip, cosmetic area | Tooth-colored bonding | Rebuilds missing corner with resin | 1 | Easy | 3–7 years | $150–$400 |
| Broader chip or discolored front tooth | Porcelain veneer | Sheaths the front surface | 1–2 | Easy | 10–15 years | $900–$2,500 |
| Lost cusp or mid‑depth crack | Inlay/onlay (porcelain or zirconia) | Rebuilds the missing portion | 1–2 | Easy to moderate | 10–15 years | $700–$1,500 |
| Large break, tooth still alive | Full crown | Caps and protects | 1–2 | Moderate | 10–15+ years | $1,100–$2,000 |
| Deep crack with nerve pain | Root canal + crown | Calms infection, restores strength | 2 | Moderate | Long-term with crown | $1,800–$3,200 total |
| Tooth split or root fracture | Extraction → implant/bridge | Replaces non‑restorable tooth | 2–5 | Moderate | Decades with care | $3,000–$6,000+ (implant total) |
Small chips: quick, natural fixes
For small chips that don’t reach the dentin, light reshaping may be all you need. If appearance matters, bonding layers color and translucency so the mended spot disappears. It’s a conservative choice.
- Why people like bonding:
- Looks natural when polished well.
- Done in one visit.
- Simple to touch up if it chips later.
Moderate fractures: onlays, inlays, and veneers
When more structure is missing, an onlay reinforces the biting surface without covering the entire tooth. Veneers shine for front‑tooth cosmetics when edges are compromised but the back of the tooth is strong.
- Choosing wisely:
- Onlay = strength with less drilling than a full crown.
- Veneer = best for front teeth that need color and shape control.
- Both can be made same‑day with CAD/CAM in some offices.
Big breaks: crowns that protect for the long haul
If a large portion of the tooth is gone, a crown adds a 360‑degree helmet. Common materials are porcelain‑fused‑to‑metal, zirconia, and lithium disilicate. Your dentist will choose based on your bite forces and aesthetic goals.
- Good signs for a crown:
- You’ve lost a full cusp or more.
- You clench or grind and need strength.
- There’s a history of cracks in that tooth.
When the nerve is involved: root canal plus a crown
If the crack exposes the pulp or infection has started, a root canal cleans the inside and seals it. Pain relief is often dramatic. A crown then prevents future splitting.
- Clues you may need a root canal:
- Lingering pain to cold or heat.
- Night pain or spontaneous throbbing.
- Gum swelling or a small pimple‑like bump next to the tooth.
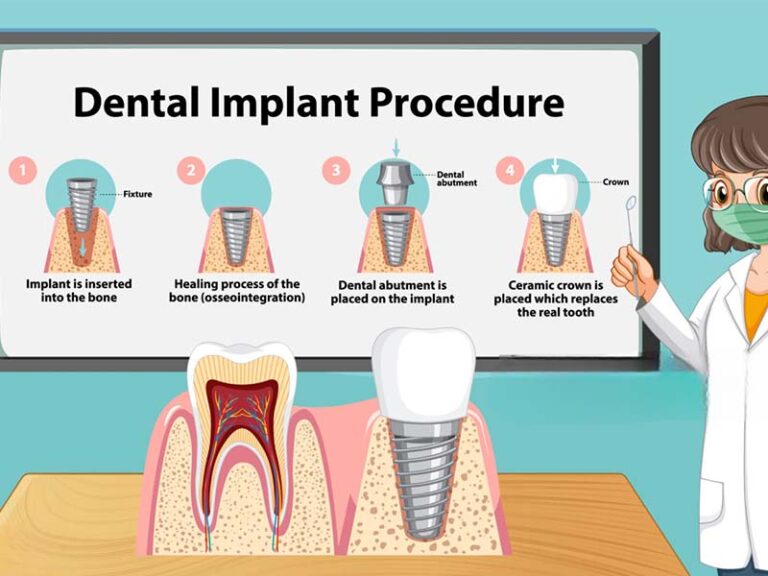
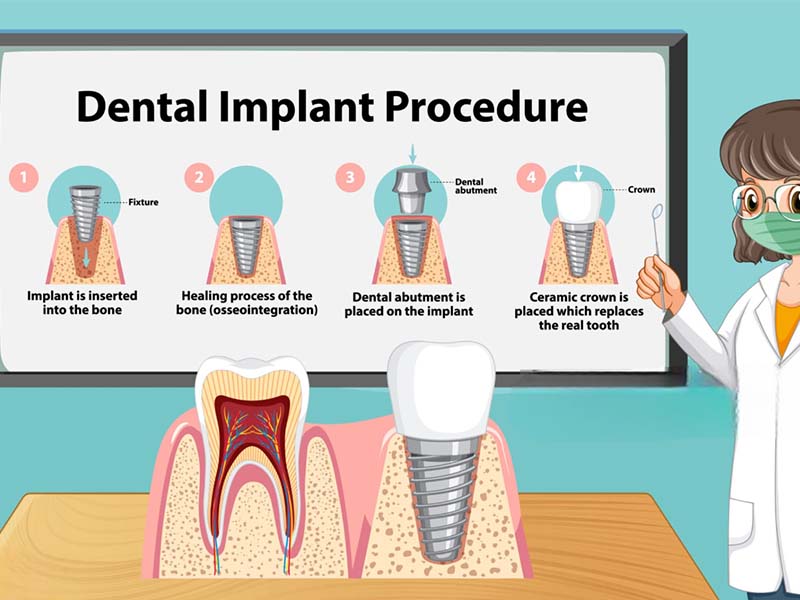
Breaks below the gumline: what if it’s “too deep”?
Fractures under the gum can still be saved if enough solid tooth can be brought above the gum. Options include crown lengthening surgery or orthodontic extrusion to “lift” the tooth a millimeter or two. When a crack runs vertically down the root, removal is usually the safest route.
- If saving the tooth isn’t realistic, replacement options include:
- Single dental implant.
- Fixed bridge using the adjacent teeth.
- Removable partial as a temporary or budget option.
Reattaching a broken piece: it’s possible
If you have a clean fragment, bring it in. Dentists can sometimes bond your own piece back and then protect it with a veneer or crown. This preserves natural translucency.
- Transport the fragment:
- Keep it moist in milk, saline, or saliva.
- Do not scrub the fragment.
- Wrap in clean plastic if no liquid is available.
Kids and broken teeth
Baby teeth are treated differently from adult teeth. Small chips are smoothed or bonded. For deeper breaks, stainless steel crowns protect chewing teeth fast. For permanent teeth in kids, preserving pulp vitality is a priority.
- Pediatric options your dentist may discuss:
- Protective cap for baby molars.
- Pulp therapy (vital pulp treatment) for deep but reversible injuries.
- Resin infiltration or sealants for craze lines.

Pain and sensitivity: what helps now
Sensitivity after a break is common. It usually comes from exposed dentin tubules or a bruised ligament. Most short‑term pain settles after the tooth is stabilized.
- Short‑term relief tips:
- Brush gently with a soft brush and warm water.
- Change to a toothpaste formulated for sensitivity.
- Use acetaminophen or ibuprofen as directed, unless your healthcare provider has told you not to.
- Skip very hot or cold items and steer clear of hard foods.
What a typical visit feels like
You’ll review what happened and what you feel. Photos and X‑rays come next. Numbing gel and local anesthesia make the visit comfortable. Many offices can 3D‑scan your tooth instead of using putty molds.
- Expect a simple flow:
- Diagnose and discuss choices with pros/cons and costs.
- Stabilize sharp edges right away.
- Do the definitive repair, sometimes the same day.
- Leave with aftercare instructions and a plan.
How long do repairs last?
Longevity depends on crack depth, bite forces, grinding habits, and hygiene. Conservative fixes like bonding are easiest to touch up. Stronger fixes like crowns or onlays protect teeth that have already shown weakness.
- Care that adds years:
- Nightguard if you clench or grind.
- Regular cleanings and checkups.
- Fix small chips promptly to prevent bigger breaks.
Costs and insurance: making smart choices
Insurance often covers a portion of medically necessary repairs, especially when a tooth is cracked or painful. Cosmetic‐only fixes get less coverage. Pre‑authorization helps avoid surprises.
- Ways to lower cost without lowering quality:
- Ask if a direct resin onlay can temporarily protect the tooth until you budget for porcelain.
- Consider same‑day CAD/CAM to reduce visits.
- Use HSA/FSA funds and ask about in‑house membership plans.
Prevention that actually works
Teeth crack under repeated stress. Spread the load, reduce extremes, and keep enamel strong. Small daily habits matter more than one big change.
- Do more of this:
- Wear a custom nightguard if you grind.
- Use a sports mouthguard for contact sports.
- Cut hard foods small; avoid chewing ice and pens.
- Treat dry mouth and acid reflux to protect enamel.
Quick myth‑busting
Not every crack means extraction. Not every ache means a root canal. And not every crown looks bulky. Modern materials are thin, strong, and lifelike.
- Three myths to forget:
- “If it doesn’t hurt, it’s fine.” Silent cracks can spread.
- “A crown fixes any crack.” Some need a root canal first; some can’t be saved.
- “Implants always hurt.” With planning, most patients report mild soreness.
Fast answers to common questions
- How quickly should I see a dentist? Same day for significant pain, swelling, or an avulsed (knocked‑out) tooth; within 24–72 hours for most chips and cracks.
- Will it be painful? With effective numbing, most treatments are quite comfortable. Any soreness is typically mild and brief.
- Can a cracked tooth heal on its own? Enamel doesn’t regenerate. Stabilizing the tooth helps stop the crack from progressing.
- What if I’m pregnant? Urgent dental problems can be treated safely during pregnancy. Let your dental team know so imaging and medications can be tailored.
Bottom line
A broken tooth can be repaired. The right plan safeguards your smile now and helps you avoid future trouble. If you’re unsure how serious the break is, call a dentist and describe what you feel and see. A steady, informed first move is enough to get you on track.
This article is for education, not a diagnosis. If you’re uncertain—or hurting—book an exam with a local dentist.